
- Intro
- November 1957 | Registered Nurse Goes to the Mattresses
- May 1958 | Cruelty in Maternity Wards
- December 1958 | Even More Cruelty In Maternity Wards
Intro
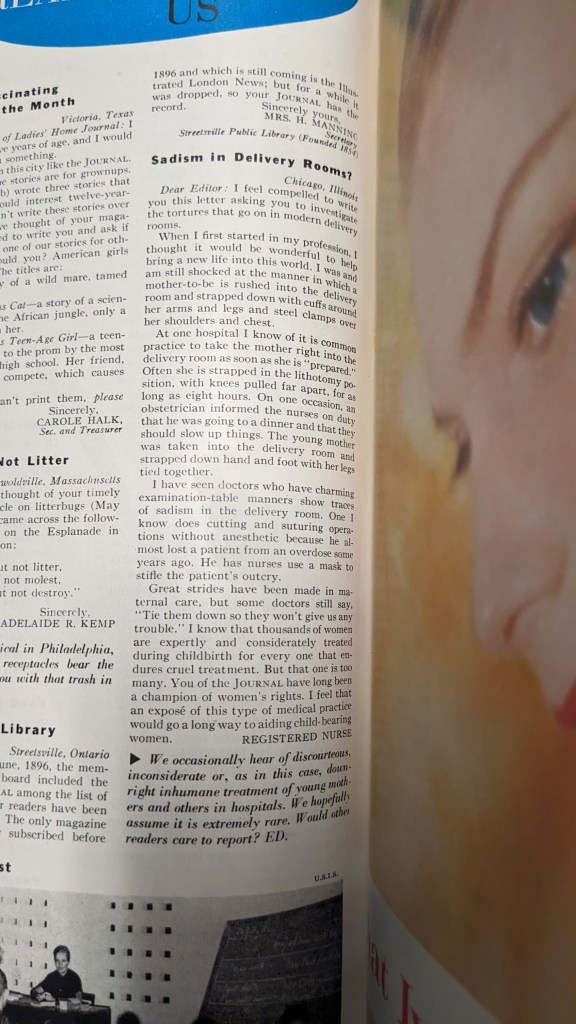
In November of 1957, a Registered Nurse wrote into the Ladies Home Journal asking them, in light of their support of women’s rights, to investigate what she called “sadism in the delivery room”.
The editor followed the letter with a brief note asking readers to write in with their experiences. Thousands of letters came in. Ladies Home Journal followed up by publishing two articles in 1958 discussing the issue and sharing many of their reader’s stories.
If you would like to share your own birth experiences, please leave a comment or send me a message– and please let me know if you would be comfortable with me sharing the story in a future post. I would like to know if the issues brought up by the mothers almost seventy years ago bare any similarity to what is experienced today.
Background, What Caught My Interest
In the read along of Trends in Obstetrics from 1950, the authors examined the trend for natural birth: that is, childbirth without drugs to reduce pain and without interventions like episiotomy or forceps and ideally in a more natural setting like at home. Especially if “home” was in a developing nation or indigenous community, as the trends promoted the idea that “primitive” women had easier births and faster recoveries– an idea the authors of the article strongly rejected citing the fact that black Americans, who due to poverty and hospital segregation, had their babies in more “primitive” situations and experienced three times the mortality rate as white Americans. Their conclusion was that modern obstetrics, having significantly reduced maternal and infant mortality was superior to so-called natural childbirth.
The article promoted modern obstetrics as a beacon of hope, the promise of better living through science, and that hospital birth was akin to a vacation for mothers (postpartum stays were 9-14 days). Based on their article, they seemed very considerate of women and their experience of childbirth. They made it clear that the survival of women and babies was the bare minimum and that good obstetrics must involve itself in the psychological well-being of mothers and babies too. They chastised authors who claimed certain practices (nursery care, bottle feeding, pain relief in labor) might lead to permanent damage of their babies, because the claims might cause women fear.
Yet, when it came to defending the routine use of episiotomy they used the threat of brain damage or death to the newborn for not using it because of the extra time it took for the baby to be born (around 15 minutes). The hypocrisy may have been overlooked by those who saw surgical interventions as necessary but it was indicative that hospital birth, hospital routines, and “sound obstetric practice” may not be as concerned with psychological well-being, or even of science, as obstetric medical professionals wanted to believe.
It was of course, an article by doctors for medical professionals (published in JAMA) about ideas from popular magazines and books for general audiences.
The elephant in the room was:
Why, if modern obstetrics was so great and provided such an improvement in mortality rates, plus cleaner and more comfortable birthing experiences for women in so short a time (really, within a generation for most, as Ladies Home Journal notes), there would be a trend for more “natural” births in the first place?
And that is where today’s read-along comes in.
November 1957 | Registered Nurse Goes to the Mattresses
In November of 1957, the Ladies Home Journal published a short but pointed letter from Registered Nurse asking them to do an investigation of “Sadism in Delivery Rooms”. The editorial staff of the journal hoped that that what she described wasn’t common and asked readers to write in telling their experiences.
Prepared
Registered Nurse (and the LHJ) used the term “prepared” very delicately, but I think it’s important to understand what went into it. While individual experiences may vary the general “preparation” for women in childbirth at this time was to separate the woman from her husband or whatever friend or family member was with her. Then get them out of their clothing and accessories and into a hospital gown and/or robe. This bit of depersonalization is common for patients to this day, though, I can understand that hospital gowns are intended to be accessible for hospital procedures and it’s better for everyone if personal effects are secured if you may or may not be unconscious, or have arms and legs bound for however many hours.
Then, pubic hair would be shaved off by a nurse. Over the years, I have read a lot of accounts of childbirth and what surprised me (considering that I learned about bikini waxing in middle school) was how particularly demeaning it was for women of this era to have their pubic hair removed. Many women said that their pubic hair was a symbol of their maturity and their womanliness. They felt infantilized and ugly with it gone. And it was only for the convenience of the doctor, just like the lithotomy position itself (but more on that later). If you have never shaved down there, it may be hard to understand how uncomfortable it would be to have a stranger attempting it, on a likely full bush, plus many accounts complained of the nurses being rough and rushed, of dry shaving, and then having freshly shaved, incredibly sensitive, probably knicked-up, skin doused in whatever antiseptic was on hand: iodine, rubbing alcohol, or listerine were all mentioned in the various birth stories I’ve heard and read from the era.
Following the nonconseual single-blade brazilian, an enema was administered, with many women not allowed to get up and go to toilet but forced to poo into a bedpan (in one letter to LHJ a mother complained that she was made to do this while nurses and a male intern watched). In the patient education film (above) that I showed a segment of in the read-along video, which dates from 1950, the male narrator explains the enema would “clear the way” for the baby to be born… as a joke we might wonder if the narrator or writers of the film understood where babies actually come from.
Historically, pooing was seen as sympathetic to childbirth. Why? Most folks with a uterus can attest, when you have menstrual cramps or labor contractions, there is a high probability of endless pooing (or so it seems). This is because of prostaglandins, which trigger uterine cramping also cause bowel cramping or peristalsis which leads to bowel movement(s). This can be a huge relief for heavily pregnant women as they often deal with constipation (and hemorrhoids). In seeing or experiencing this normal physiological change around menstruation and childbirth, the idea got around that causing a woman to poo might get labour going: so we have clysters (enemas) and laxatives (such as castor oil or Taco Bell) recommended in medical literature from antiquity and in folk remedies to the present day. While stimulant laxatives can cause uterine contractions but they don’t actually start or augment labor. Unless directed by a qualified medical professional, its best to avoid them.
I’m sure that every maternity ward had their own justification for the practice, but the real utility of giving women enemas as routine childbirth prep was to prevent the precious doctor from getting shat on during delivery, effectively disarming the bound woman’s only defense.
In some cases, women reported having a catheter placed to collect urine to prevent patients bothering nurses to use the toilet. This may have been how some of the women who reported being bound for hours in the LHJ articles were “prepared”. All of these preparations, while they may have been considered standard and necessary (if only for the convenience of the doctor and nursing staff) they were invasive, demeaning, and uncomfortable.
And for most, the “veritable hell” had only just begun.
May 1958 | Cruelty in Maternity Wards
Thousands of letters came in following Registered Nurse’s letter. Ladies Home Journal published “Journal Mothers report on Cruelty in Maternty Wards” in May of 1958, written up by Gladys Denny Schultz, quoting extensively from positive and negative birth experiences from mothers, some of whom were doctors and nurses themselves, as well as letters for and against certain practices from doctors and nurses, and the author includes the medical consensus regarding certain practices.
One of the first accounts, under “How to Make Childbirth a Joy” the mother says that having her husband with her until the moment of delivery made all the difference, and that she had such wonderful supportive nurses and doctor. But what I noticed was the lack of patient information, she believed that she didn’t have any anesthesia because she didn’t need any in such a great environment– but she said that she was given a “rubber apparatus” to hold in her hand and take a whiff of when she was too uncomfortable. Most likely she was being given nitrous oxide, which is an anesthetic, and that’s why, to her “amazement” she was able to carry out a conversation through delivery. But I am happy, in spite of her not giving consent for pain drugs, that she felt she had a good childbirth experience after two terrible ones.
Abuses Confirmed
All of Registered Nurse’s claims were confirmed by women right across the country: labouring women restrained for hours in the lithotomy position in delivery rooms, unattended; women having their babies artificially held back for the doctor’s convenience; and cutting and suturing done without anaesthetic.
Horrifyingly, “fully half” of the women reported having their babies artificially held back for the doctor’s convenience, by having their legs tied together and being given anesthetic (which reduces uterine contractions). Being already bound by their hands meant that these women were completely helpless against nurses strapping masks to their faces, injecting them with other drugs, and tying their legs together, even sitting on them. (More on this in part two, below.) Many reported being slapped, choked, and threatened with dead or disabled babies for being too loud or asking for assistance. Sadly, many women said they didn’t have any reason to believe other mothers were treated any better, until they read Registered Nurse’s letter.
Justifications
The justifications provided by medical professionals ranged from blanket denials to “sound obstetrics” to “actually, it’s not that bad” to hospitals being understaffed by overworked doctors and nurses. And there is something to this: the baby boom occured at the same time that hospital birth was becoming ubiquitous. The facilities weren’t fit for purpose and there simply weren’t enough trained doctors or nurses– often, the doctor delivering the baby wasn’t an obstetrician but a general practitioner and the nursing staff weren’t trained for obstetrics.
The Journal pointed out that nurses were not allowed to report or criticize doctors or hospital routines if they wanted to keep their license, and that they shouldn’t be blamed for the things they did because they were just following orders. Perhaps this was a serious scalding burn on nurses doing sadistic, dangerous things to patients and their babies because every person of their generation should be very well aware of the Nazi trials, and the excuses that Nazi atrocities were a matter of “following orders”. But perhaps, in a deeply concerning way, Gladys Denny Schultz actually thought that way. I hope not. Between potentially killing someone’s baby (while torturing a laboring mother) and losing my job? That’s an easier choice for me than what shoes I am gonna wear today. And I lost count of the number of times the nursing shortage was brought up in the article, it’s not as if it would be difficult to find another job.
Why Restraints? | My Theory
The medical justification of the practice of restraining women was that it was the only way to prevent contamination of the sterile field, the sterile field produced by draping the woman in cloth. The threat given was that infection used to kill lots of mothers and babies, and only by restraining the arms and legs can we preserve the sterile field and prevent infections.
Forgive the language but I call bullshit.
By the 1950s, doctors understood what caused infections and they knew how to prevent them with hand washing and antiseptics, and they had antibiotics in case infections developed. If they were really concerned about the mother’s arms, hands, or legs infecting the baby, the rational thing to do would be to add an antiseptic shower to the already invasive prep routine. But my theory is that the sheets and the restraints were never really about preventing infections…
Women began to be restrained in labor and during delivery in the early 20th century, as more anesthetics were being developed for use during childbirth, anaesthetics which often had the side effect of causing women to flail about, hallucinating. One mother, cited in the Ladies Home Journal, in September 1914, after a scopolomine birth reported
“But though I slept quite soundly and peacefully and knew nothing at all of what was going on about me, I was nevertheless behaving very badly […] for they afterward told me that I had had a perfect wrestling match with the head nurse.”
Frau Anna Straub, “The Painless Childbirth” Ladies Home Journal, September 1914
To protect the mothers themselves and the staff, and knowing the patient was effectively unconscious, hospital routines were established involving restraining women and then leaving them alone (they understood that less stimuli = less freaking out) until delivery was imminent.
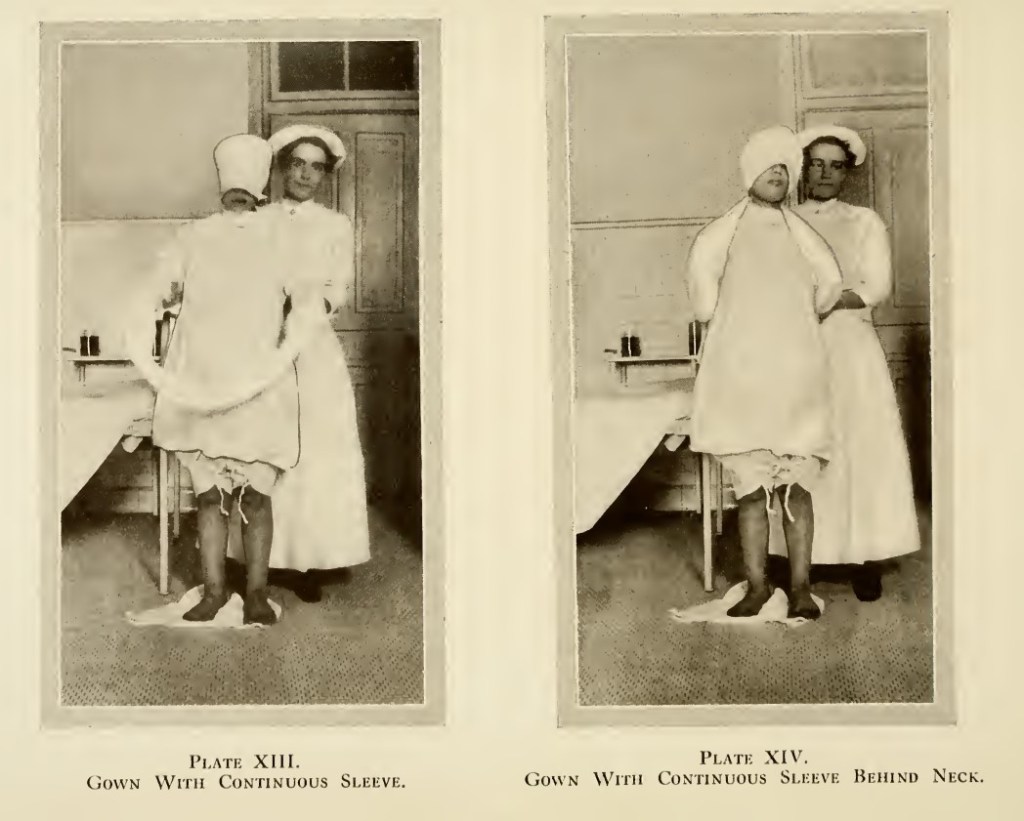

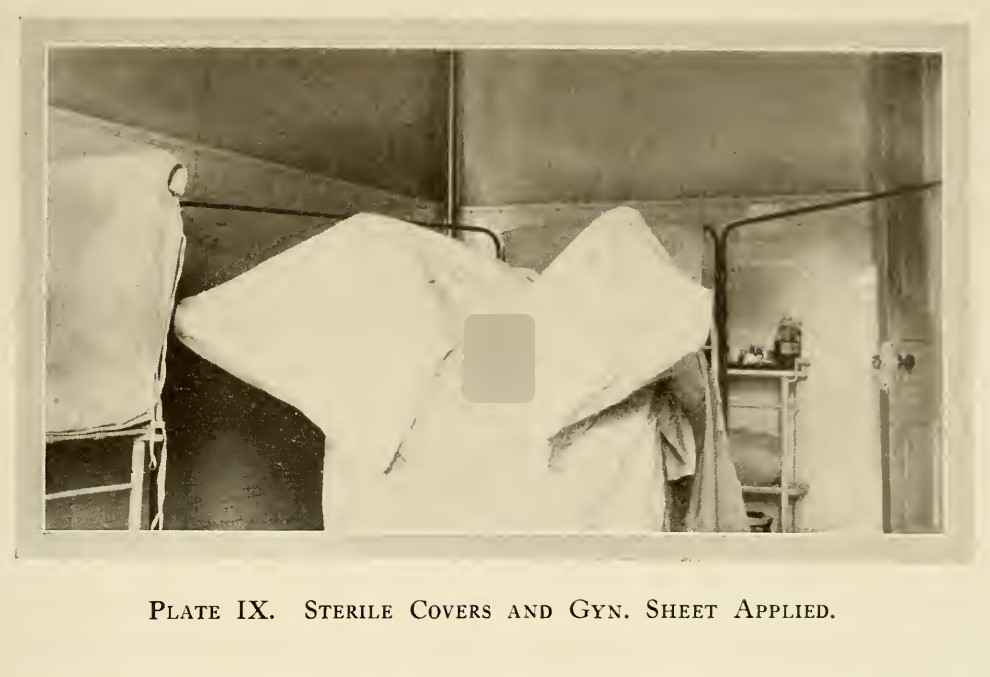
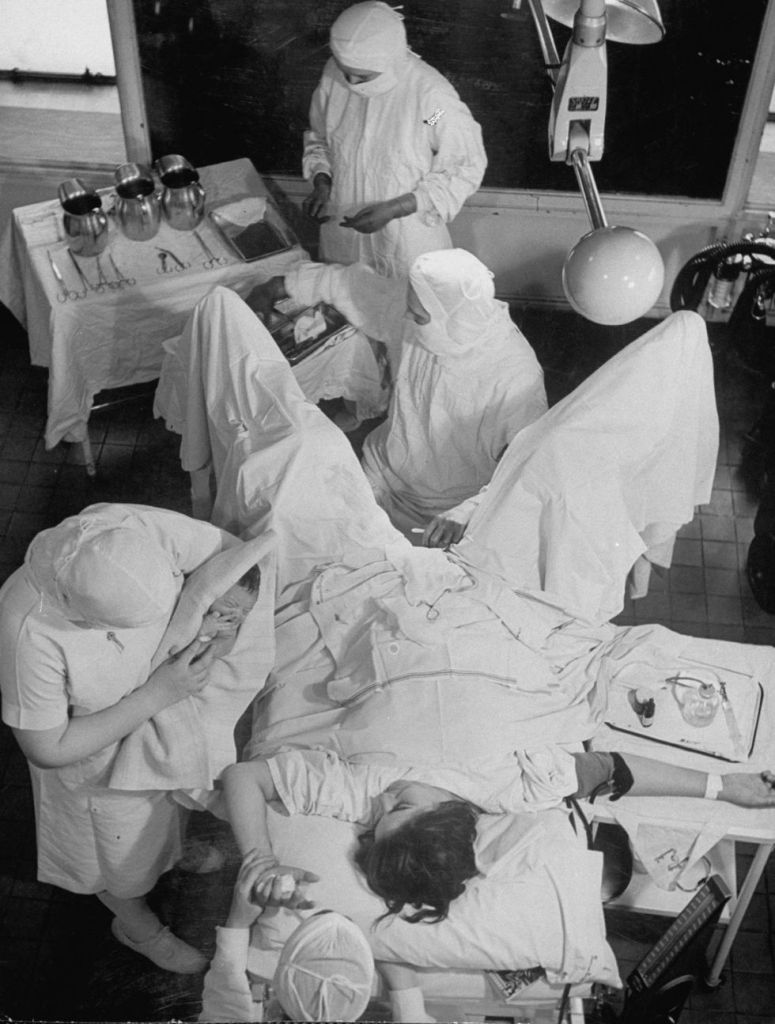
Above images are from Bertha Van Hoosen’s 1915 book Scopolamine- Morphine Anesthesia. The patient is restrained and left alone until delivery was imminent, then restrained in the lithotomy position and draped with sterile cloths. This was a time before antibiotics and limited antiseptics. The “sterile drapes” may have done something but seem more likely to be a means of dehumanizing (possibly desexualizing) the woman who is giving birth. It’s just a vagina (interestingly, unshaved), and not a person.
Or maybe the cloths were just traditional.
For centuries, male physicians were taught how to examine female patients who were draped in or hidden behind cloths. (Poor pregnant women were such a boon to the profession, as they couldn’t insist on modesty– because they couldn’t afford it.) This “sterile drapes” thing seems like a pseudo-scientific excuse to continue with that tradition– and so does restraining women’s arms and legs during delivery, along with leaving them alone during labor.
However, restraint wasn’t as universal a practice as draping: in the 1950 patient education film, the patient was shown handles to grip during delivery. In the photo above, labeled as being from the 1940s, shows a woman with her arms free. Perhaps this is due to the use of restraints being for the relatively new and (in the US especially) controversial purpose of obstetric anaesthetic. Perhaps where the adoption of scopolomine was promoted, a tradition of restraining women became entrenched; where it was rejected, women were only expected to have legs in stirrups for the longer standing and more universal traditions of draperies and lithotomy position.
Of course, this is just my theory and I need to do more research. For example, I would like to know if male patients undergoing procedures with a risk of infection/ need to “maintain a sterile field” were also put into restraints where maternity patients were. If you have ideas or information about this, I would love to hear from you.
What About Homebirths?
One mother said that her next birth would be at home because she just didn’t think the emotional disadvantages of a hospital birth were worth it:
“Many normal deliveries are turned into nightmares for the mothers by ‘routine’ obstetrical practices. I have had two such experiences. My third baby will be born at home, despite the sterile advantages of a hospital confinement, for I feel the accompanying emotional disadvantages are just not worth it.”
Columbus Ohio mother, “Journal Mothers report on Cruelty in Maternity Wards” Ladies Home Journal, May 1958
But the article explains the majority of doctors at the time wouldn’t agree to attend a home birth, and for women with higher risk births, LHJ were absolute in saying that hospital births were necessary. The tide for American women (at least white women in segregated areas) had shifted completely in a generation. In The Great Chicago Baby Mix-Up, in 1930, only about half of women in the city of Chicago had a hospital birth. Less than thirty years later it was almost impossible to have a home birth– and at the same time these horrors were going on in many maternity wards. Gladys Denny Schultz worded it in an interesting way,
“Today most women in comfortable circumstances are required to go to hospitals to have their babies.”
Gladys Denny Schultz, ibid.
Comfortable circumstances. I suppose she meant economics and potentially race, though then and certainly now, economics has more to do with, well, everything. If you were in uncomfortable circumstances, say, living in a tin shack 100 miles from the nearest town, you were the type to have a homebirth. That’s certainly the angle that was played up in anti-midwifery propaganda during this time. In the December article a nurse brings up childbirth in “the country”, where women were still expected to go to the hospital to give birth, and often found themselves having babies artificially held back until the doctor could get there.
Suffice to say home birth wasn’t a feasible option for most American women in the 1950s. How could hospital birth be made better?
Practicable Solution | Husbands
Many of the mothers wrote about wanting to have their husbands with them during labor, one praised a doctor who allowed a husband to stay with his wife for the birth even though it was against hospital rules. Others talked about begging staff to allow their husbands back and were refused or ignored. When one husband asked the doctor about the bruises all over his wife’s face, neck, and arms (from being slapped and choked by a nurse) the doctor told him that women beat themselves up during labor. No doubt, if he had been present, and if Nurse-y had dare lay a hand on his wife in anger, she only would have done it once.
“Just let a few husbands into the delivery rooms and let them watch what goes on there. That’s all it will take– they’ll change it!”
Former Teacher, Detroit, Michigan
The Journal agreed. This one change in hospital routine would eliminate all the abuses and cruelty without requiring any more work from limited hospital staff. In the article, they pleaded with medical associations and hospitals to reconsider the general ban on husbands in L&D.
They also had suggestions for expectant mothers, including shopping around for obstetricians as well as subtly suggesting that women name and shame abusive or dangerous doctors or hospitals to their friends and acquaintances. But most importantly, understanding that medical professionals were not allowed to report abuse, that patients must report any abuse or cruel treatment that they experience.
After this article was published, even more letters were sent in, so many that Ladies Home Journal felt they must do another article… which will be the subject of the next read along.
December 1958 | Even More Cruelty In Maternity Wards
In December of 1958, Ladies Home Journal published a follow-up article as the letters continued to come in. This article featured fewer letters but the stories they highlighted were all the more poignant, one was so horrible I added a second content warning ahead of it in the video. Suffice to say that, in my opinion, a doctor who commits infanticide to get to a dinner date should spend the rest of his life in prison.
While the first article focused on raising awareness of the issue, to see if the claims made by Registered Nurse were substantiated by their readers, this article focused on the denials or justifications made by medical professionals with a warning that abuses suffered by women in maternity wards was creating a gulf between lay people and the medical profession as a whole. The Ladies Home Journal hoped that by bringing the issues to light and with their suggestions that gulf could be bridged from each side, making the experience of childbirth better for everyone involved.
The Claims of Medical Professionals
First, the claims by medical professionals regarding the stories of cruelty:
- Blanket Denial: they never saw it, they never experienced it, so it’s not occuring.
- The women complaining are spoiled, hysterical, ignorant, fearful, and have unreasonable demands. (The Karen Fallacy.)
- Husbands are too emotionally unstable to handle staying with their wives during labor, let alone delivery.
- Women’s accounts cannot be trusted because of the anesthetic drugs.
- Hospitals are overworked and understaffed and cannot accommodate the demands of fearful ignorant women.
Other than sharing the stories of women and the justifications (rather than denials) of cruel practices by medical professionals, there’s not really much that can be said to those denying their existence simply because they didn’t have personal experience of them.
The Karen Fallacy
As to the Karen Fallacy, the journal pointed out that nearly all the women who wrote in about their bad experiences also told of their good experiences, many had four to eight children, giving birth in different hospitals with different doctors. Often, it was the difference between the good and the bad that led them to write in with their stories. As Gladys points out:
“If they were hysterical, spoiled or fearful by nature, it would seem to follow that they would report every childbirth experience as an abuse.”
Gladys Denny Schultz
Husbands
Many mothers reported that when their husbands were allowed to stay with them they needed fewer drugs and labor seemed to go by faster, they were useful in supporting their wives during childbirth– making the job of hospital staff easier (assuming it was the kind of staff that checked on and actively cared for laboring women).
“Judging from our letters, husbands do not seem to be so frail as the professionals indicate. Mothers who had their husbands with them report no casualties.”
Gladys Denny Schultz
Fathers too, wanted to be part of the experience, reporting “that they found it a deeply spiritual experience, increased immeasurably the tenderness they felt for both wife and baby.” However, the journal pointed out that it was important for fathers to be self aware about their own limitations: if they knew they were unfit for graphic medical situations or were emotional drinkers, for example, they ought to avoid the labor and delivery room.
Drugs
It is a fact that the anesthetic drugs commonly used could cause hallucinations and erratic behaviour, however, Gladys points out that many women reported cruel treatment without or before the use of drugs and others reported great experiences while on drugs. More concerning was the use of drugs on non-consenting women, particularly those actively refusing drugs, or drugs given without warning while the abuse was taking place, for example, most women reported that when the baby was crowning and the doctor wasn’t there, as nurses were tying their legs together, someone was putting an ether cone on their face, or slapping an ether soaked bandage over their nose. Yes, ether reduces contractions but I can’t help but wonder if it wasn’t part of the “don’t believe what they say, it’s the drugs talking” defence.
“They put an ether cone over my nose and forced my legs together […] I did not hear the baby’s first cry”
Mrs M. S.
“Finally one of the nurses came in and without a word lay down across my legs to hold the baby back. She then slapped a bandage containing ether across my nose.”
Mrs D. L. M,
Forcibly Holding Back Babies | My Theory
In both articles, the issue of hospitals being overworked and understaffed was brought up repeatedly by Gladys, the mothers, and the medical professionals. The ethical folks said it likely contributed to abuses but that it wasn’t an excuse– in this article, however, one nurse wrote in to explain why babies were artificially held back without an intention to be cruel. She explained that it mostly happens in country or small-town hospitals where there’s only one doctor and they have to drive in from 15-30 miles away.
“If the nursing staff is small, inadequate or poorly trained, as is common, a doctor may feel that holding back the baby is a lesser evil than a torn birth canal, a sudden hemorrhage or a cyanotic baby when there is no one around to handle such an emergency. I am not defending the practice, mind you. I am just explaining how such a thing can occur without everyone concerned being a sadist.”
A Registered Nurse
I wasn’t sure why nurses were holding back babies until a doctor or a specific doctor arrived. I thought it had to do with something like commission because, as Gladys goes on to explain, this practice was by no means limited to small-town or country hospitals, but big teaching hospitals in metropolitan areas with multiple residents and attendants available at any given time. However, if this is the medical reasoning then it’s far more sickening, which even now I can hardly believe is possible but the facts are there.
When I was doing research on vagitus uterinus it was necessary for me to get my head around the historiography of obstetrics at the time, the late 19th and early 20th century, since it was being reported in the most prestigious professional journals of the time. These case reports were being written and read and commented on by the most experienced obstetricians with the most cutting edge technologies and techniques. What did they know and believe about childbirth? When the baby is ready to be born it needs to GTFO ASAP so it doesn’t asphyxiate and die: with the water broken and the baby in the birth canal, lord knows what the cord is up to or the placenta… jesus take the wheel.
By the 1950s, doctors, medical professionals (whatever their training), likely the mothers and fathers too, the janitors even, they all understood that preventing a baby from being born even for a moment– god forbid the extra 15 minutes that an intact perineum might require— was to risk the life of the child. Therefore, forcibly holding back a baby from being born because there’s a potential for a complication that the staff aren’t prepared to handle is an intentional choice to cause a “stillbirth” rather than accept responsibility for handling post-partum complications. That’s exactly what happened in Mrs J.R., who was giving birth after three miscarriages, only to have the nurses ignore her shouts and calls for help for an hour after her water broke and then discovered her doctor had left on vacation without leaving contact information.
“Finally they crossed my legs and gave me ether, because my doctor could not be located. I awoke on the delivery table, and realized my stomach was flat. I asked the doctor what I had had. He replied calmly, ‘It was a girl.’ I was told that she had been choked by the cord.”
Mrs J. R.
The medical staff coordinated their efforts to make the mother’s body the cause of the baby’s death. It’s unforgivable. Mrs J. R. must have been a very strong woman, she went on to try again for a baby and was able to give birth in a much better environment- with supportive nursing staff and a competent and considerate doctor. “Thanks to my second doctor, I have a wonderful life.” I wish that all obstetricians and L&D nurses would recognize that another day at work for them can make or break their patient’s entire life. I believe that the majority of them do. The job description should go far beyond mere survival, but make no mistake, survival is the lowest possible bar for an obstetric medical professional.
Alive But Damaged
Dr John Whitridge Jr said that improvements in mortality rates weren’t good enough, maternity care needed to consider the patients’ well-being. Many people who wrote expressed concerns about the sanity of mothers and the brain damage of children caused by the maternity ward abuses,
“Oh, yes, let us build big mental hospitals for seared mothers, and schools for retarded children. Some of this could be prevented right in the labor and delivery room.”
Mrs M. S. [“retarded” was a legitimate medical term at the time ]
The first letter of the article was about Danny, a little boy who was mentally disabled due to being artificially held back at birth.
“Danny is the victim of a delayed delivery. He suffered a brain injury from lack of oxygen at birth. Now, nine long years later, we are learning to accept the results of imprudent, thoughtlessly administered anesthetic while nurses waited for a doctor to come.”
Name Withheld
A registered nurse wondered at the fact that while other fields of medicine were becoming more concerned with patient mental well-being, childbirth was moving in the opposite direction,
“Why obstetrical care seems to be becoming increasingly mechanical and hospital- rather than patient-centered when other branches of medicine are concentrating on the psychosomatic side of illness, is a paradox.”
Mrs E. E. S., Registered Nurse
In the May article, a reader reported hearing nurses tell women who were in distress, “You had your fun, now you can suffer.” In the December article, Mrs W. S. B. noticed the difference between being a general hospital patient and being a maternity patient
“I believe there exists among nurses a definite hostility toward women in childbirth. I have been in hospitals for other reasons and have been treated with the greatest consideration. There seems to be a feeling that a woman in childbirth has brought her troubles on herself and so deserves no kindness. One moaning in pain from an operation is an object of sympathy. A woman moaning with pain in childbirth is just a nuisance.”
Mrs W. S. B.
There was something rotten in maternity care and a young psychiatrist noticed it,
“In the prenatal clinics and in the delivery room, I have gradually become aware of the strikingly negative attitude with which the women are handled. […] Unless we [..] perceive that pregnant women are human beings in a state of physiologic and psychologic flux, we, as physicians, must accept part of the responsibility for the resentful mother and the unloved child.”
Dr Myron F Weiner
Cog in the Machine
In both articles (and in many books written about American childbirth since), the phrases “assembly line” and “cog in a machine” were used frequently. Patients were made to feel like they weren’t human, some said they felt like a trapped animal. Perhaps it comes from the focus on efficiency of the previous generation (it’s like the focus on decluttering for my generation) bleeding into how maternity wards were run. In the US, maternity units were and are businesses and even today many families complain that it felt like the point of every rule and intervention was to rack up the highest bill possible in the shortest amount of time, then to get the room ready for the next patient.

Solution | Nurse Midwives
Of course, when a system isn’t fit for purpose, understaffed by underqualified people who are overworked, efficiency is all they have to cling too, there’s no room for humanity. The solution, therefore, is training more qualified medical professionals. It was John Whitrigde Jr who proposed a massive training program for nurse midwives, 400 per year rather than the then-current 40 per year. It was a rational solution to the shortage of ob-gyns and underqualified and short nursing staff in American maternity wards. Nurse-midwives would have the training to not only provide prenatal care and education, but support women throughout labor and if the doctor wasn’t available, they would be able to handle normal deliveries.
By the 1950s, the American maternity system was at the point of breaking: just as hospital births became common the baby boom was in full swing. Here was a fork in the road: make a rational compromise to bring on nurse midwives to support normal healthy pregnancies and childbirth in hospitals, while allowing OB’s to focus their specialized skills on higher risk patients- to reduce the assembly line methods that allowed for abuses to occur– or to reject rational compromised and continue with business as usual.
The choice, was of course, the latter.
The result was a widening gulf, a more extreme natural birth movement and more extreme interventionalist hospital births, resulting in part to the shamefully high maternal and infant mortality rates in the United States today. Fortunately, it seems that some progress is finally being made with regards to nurse midwives in American hospitals– nearly seventy years overdue.
If you would like to support my work, please consider becoming a patron on Patreon. Also check out my YouTube channel, subscribe, and share my videos so more people can find my work.
