

I wrote this article for the Iowa City Babywearers group blog, published on February 18th, 2018. We decided to retire the group in March of this year and our website will be expiring in November, so I thought I would salvage a few of the most popular articles and share them with TBH readers.
At a recent meeting, Sylvia* introduced us to her two and half-year-old daughter, Emily. Sylvia and her extended family are going on a vacation later this year and wanted to learn about their options for using a carrier with Emily as her custom wheelchair will not go off-road. Emily has cerebral palsy, a neuromuscular condition causing a spectrum of symptoms including difficulties with muscle tone and coordination, hearing and vision, and learning disabilities.
*names have been changed for privacy
About Cerebral Palsy
There is no cure for cerebral palsy. While symptoms become more noticeable with age the disease is not progressive. Preterm births, twins, and infants who experience difficult births, or head trauma during or after birth are most likely to have cerebral palsy. In some cases, it is caused by infection or environmental toxins during pregnancy, and in very rare (2%) cases, the cause is genetic. Nearly 80% of people with cerebral palsy have structural problems in the area of the brain that controls movement, balance, and posture; and some will experience seizures.
Babies born with cerebral palsy may seem like any other newborn, with signs of the condition not becoming noticeable until they miss sitting and crawling milestones around six to ten months of age. However some newborns with the condition may be extra floppy or too stiff, and some may already show signs of scoliosis.
Infants and children with cerebral palsy tend to experience chronic, localized pain in over-strained joints and muscles; this may make them more fussy and difficult to get to sleep. Toddlers may not be able to walk, may have trouble with drooling and swallowing– the combination is a choking hazard– and they may have trouble communicating. Non-mobile children with cerebral palsy may have weak bones, as bone density is determined by how much stress is put on growing bones, which puts them at risk of low-stress fractures.
There are subtypes of cerebral palsy which indicate the most noticeable symptoms, including spastic for stiff muscles, ataxic for poor coordination, and dyskinetic or athetoid for involuntary writhing movements; individuals may experience a combination of these types. Some may have bone or joint deformities, including scoliosis.
Treatment may include physical therapy, speech therapy, braces and assistive technology, muscle relaxers, and (in extreme cases) surgery to lengthen muscles or to cut overactive nerves. In the future, stem cell therapy may be beneficial. No two individuals with cerebral palsy will have the same constellation of symptoms or treatments.
About Emily’s Case
During her birth, Emily stopped breathing. Her doctors and her parents understood that she had cerebral palsy from birth, however, she was not formally diagnosed until she was ten months old. Today, when you first meet Emily, aside from the head of blonde curls, you’ll notice that she is actively engaging with her environment. She has trouble tracking with her eyes but her hearing is spot on and she follows voices around the room, clearly communicating how she feels with her expressive face. She loves attention, flashing a broad grin when you talk to her and she’ll furrow her brow and make an exasperated sigh when she’s getting bored. When Sylvia pulls out her breakfast, which is fed through a port in her tummy due to problems swallowing, Emily starts happily wiggling in her chair– I do the exact same happy dance when the pizza comes to the table.
Sylvia used the Infantino 4-in-1 carrier with Emily for the first year. However, Emily tends to flex her legs and arms it was difficult to get her in and out of the carrier. As Emily grew, the only position they could use was a front carry, facing in. A friend gave them an Ergo when Emily outgrew the 4-in-1, but the wide seat was too wide for her. When Emily needed to flex her legs together the wide seat prevented her from doing so and it put strain on her hips.
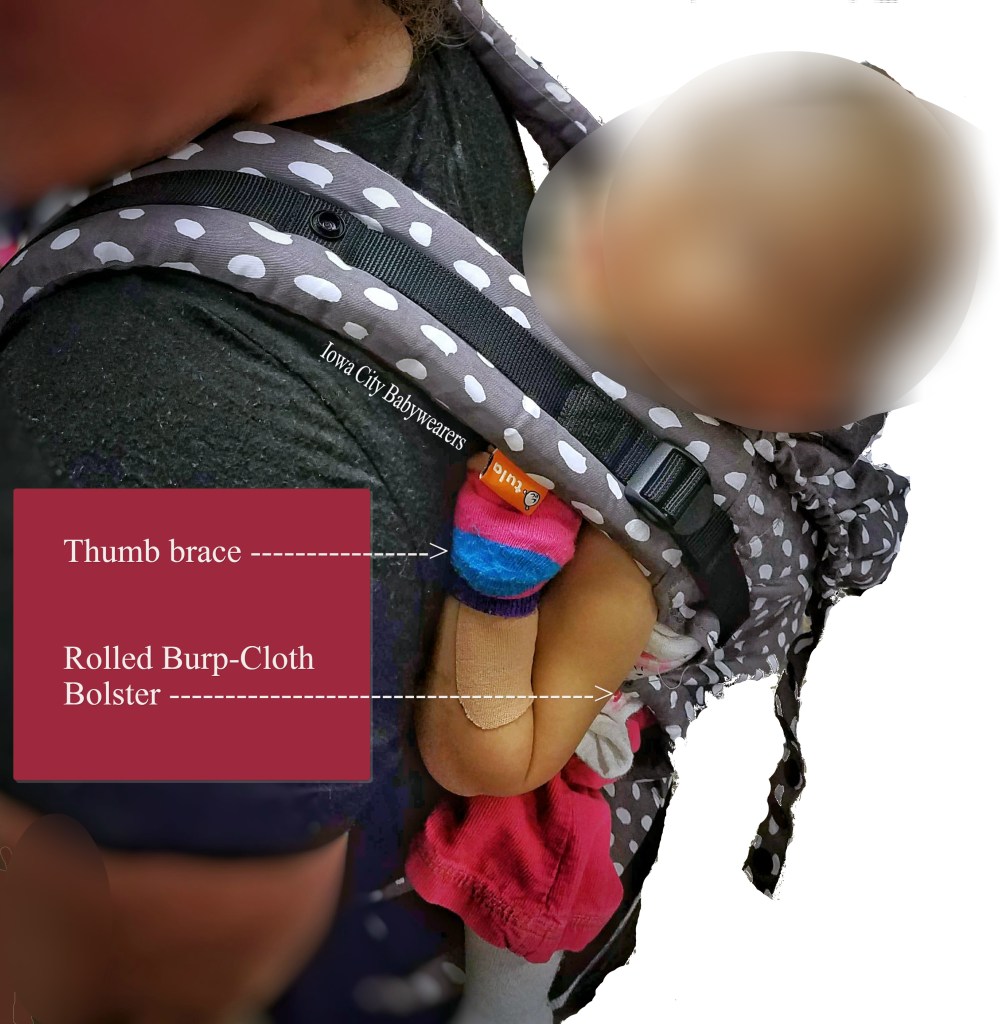
Now Emily spends most of her time in a custom wheelchair that supports her spine side-to-side (she tends to slump to the left) with a slight recline for better head support. Her legs are supported all the way to the foot straps for her feet. In addition to the feeding port on her belly, Emily has a splint on one hand to prevent her over-flexing her thumb, which is wrapped up to protect it.
“Developmentally, she is 3 to 5 months old so she is basically an infant in a long, toddler body. She still needs to be held often and with her getting heavier and heavier it makes holding her more difficult.”
Slyvia, Emily’s mom
Babywearing Help
My initial thought considering how Sylvia described Emily’s leg flexing (straight out and knees together) was a historical example of a Northern European style carry. The carrier used was similar in form to a mei-tai, but the child was placed in it sideways, with legs together hanging out (or swaddled) to one side.

Before we tried that, I wanted to see how Emily would handle a regular SSC carry. Due to Emily’s size and Sylvia’s goal of going hiking on their family vacation, we opted for a back carry. Note: the larger the child, the more your field of vision will be blocked with a front carry, even when facing in. This increases the risk of falling because you can’t see where you’re stepping.
Sylvia will always have (and need) help to get Emily on her back. This is very important because none of the options for getting a child on one’s back will work for Sylvia because of Emily’s feeding port on her stomach which cannot be dragged or slid, in addition, Emily may randomly flex her legs, arms, or both. With a neurotypical child who is flexing arms and legs, the wearer can ease the child’s limbs into position with a bit of bouncing, gravity, and tension from the carrier. But for child with cerebral palsy whose muscles can seize up, joints locked, no amount of finagling by the wearer is going to work. For as long as Sylvia wants to wear her, she will require assistance in getting Emily up and down. Fortunately, she has a very supportive family.
The first carrier we tried was a preschool-size carrier. After Sylvia buckled the waist strap, Kelsey and I helped place Emily on her back, putting her arms and legs in place while Sylvia got the shoulder straps on and adjusted. Sliding my hand inside the carrier between Emily and Sylvia, I checked to ensure that Emily’s shirt and port weren’t caught on mom’s clothes. Emily was sitting comfortably, able to flex her arms and legs but her torso wasn’t well supported enough for mom to walk without feeling like she needed to lean forward. While Emily has high-tone in her limbs, she has low-tone in her trunk and needed more support from the body of the carrier. Plus Emily’s seat was hanging over the waistband, so we tried another.
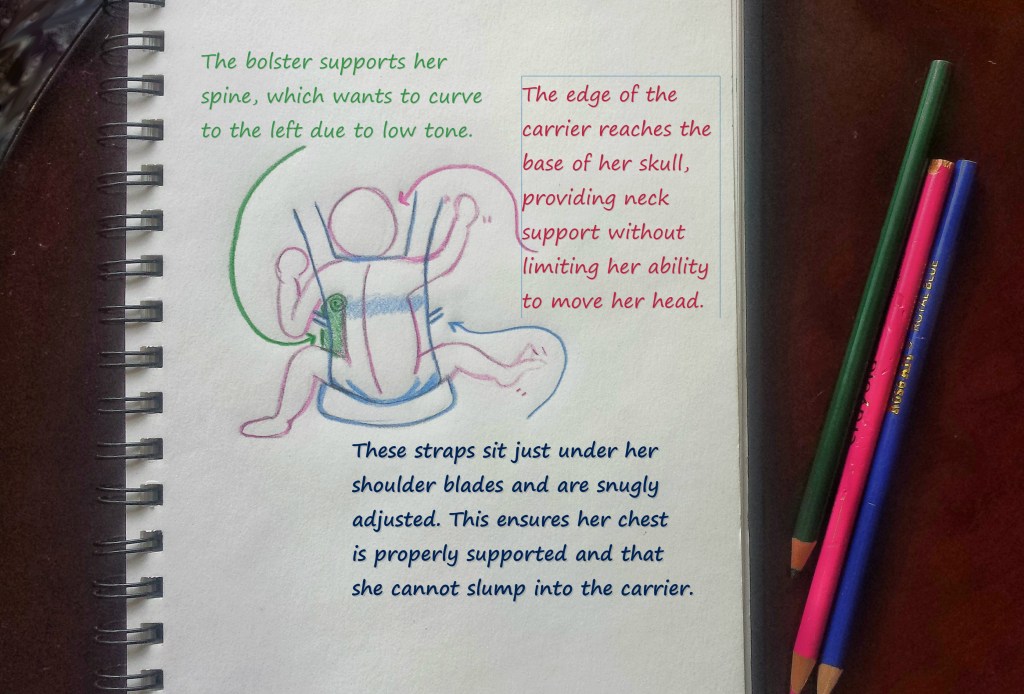
The second carrier was the Tula Free-to-Grow (photo and diagram above). We placed her in it the same as the preschooler SSC but this time the body of the carrier fitted Emily’s body much closer for better support. For a child without cerebral palsy, it may have been on the snug side, but for Emily, this was exactly what she needed. To further support her spine, we rolled up a burp cloth and used it as a bolster between the webbing of the shoulder strap and her ribs, to help prevent her left-lean.

The third carrier we tried was a toddler-sized wrap-conversion mei tai (above, rainbow stripes, made by Kelsey) with wide straps. After much patience on Emily and Sylvia’s part, Kelsey and I had found a legs-together position that provided enough support for Emily’s spine and head while allowing her to flex her legs, with knees together, and it was comfortable for mom. However, it was a front carry, so not something we recommend for long hikes but something that could work well for general holding with arms free.
Benefits of Babywearing for kids with Cerebral Palsy
Communication can be limited for people with cerebral palsy, lack of coordination of the muscles of the face, tongue, and throat may make speech impossible and the same is true for sign language. But one of the biggest hurdles is preventing learned helplessness and passive communication exclusively with caregivers. Babywearing may encourage both the child and the public to engage each other in communication simply by proximity. Even in neurotypical infants and children, being in a carrier nearer the heads and faces of people (as opposed to lower down in a stroller or carried car seat) helps children hear and see other people engaging in conversation and using body language.
The movements of being in an infant carrier may help with bone density, at least when compared to smoothly rolling in a stroller or wheelchair, as the jostling of the caregiver going about their day puts some healthy stress on the bones of the child. We already know that the movements of a babywearing caregiver help neurotypical infants and children develop core strength and coordination (Karasik 2013, 2015; Suskind), it may, in some cases, be beneficial for children with cerebral palsy. Babywearing may encourage caregivers to get kids outside more regularly, without concern for where a wheelchair can or can’t go. We know the benefits of being in nature for everyone’s well-being (adults and children alike).
“[Outside] in her chair, she’s completely exposed and it makes her upset so we can’t [go for walks] unless we are going into a building [..] she just doesn’t like to be cold and the wind catches her breath and causes difficulties breathing.”
Syliva
The chronic pain and sleep disturbances associated with cerebral palsy may be reduced with the comforting physical contact of a caregiver. Simply the body warmth provided by the caregiver’s body heat can help soothe achy muscles and joints. There is some evidence that some infant crying may be a reflex to increase body heat, much like shivering (Hofer). And there is transport response, which soothes crying infants as they are carried during a walk (Esposito). There are the analgesic properties of skin-to-skin (Gray) and for infants who can safely breastfeed, nursing may be easier with the added support of an infant carrier (and some can nurse hands-free using a carrier).
The crying associated with lack of sleep and chronic pain may be reduced by carrying (Hunizker). However, more interestingly, the caregiver’s perception of crying is altered when they frequently carry their baby: babywearing parents tend to be more sympathetic about and recall less crying than actually occurred, whereas parents who didn’t carry reported more feelings of resentment and frustration about their infant’s crying (Elliot). For CP infants with reflux that prevents them from sleeping well, the upright position of most carriers can reduce reflux and allow infants to sleep.
Comfort and Safety
It is important to emphasize that every child with cerebral palsy has unique symptoms and needs. In Emily’s case, Kelsey and I (with almost 30 years of babywearing teaching experience between us) along with Sylvia’s help spent over an hour ensuring that Emily was comfortable and safe in each carry, in each carrier. When babywearing is safe and comfortable for a child with cerebral palsy, it may improve the quality of life for parents, caregivers, and for the children themselves.
If you have experience babywearing a child with special needs, we’d love to hear your story!
Sources & Further Reading on Cerebral Palsy:
Elliot, Ruth, et al. “The Effect of different soothing interventions on infant crying and on parent-infant interaction.” Infant Mental Health Journal 23:3 (2002) 310-328.
Esposito, et. al. “The Calming Effect of maternal carrying in different mammalian species.” Frontiers in Psychology 6:445 (2015)
Gray, L. et al. “Skin to Skin contact is analgesic in healthy newborns.” Pediatrics 105:e14 (2002).
Hofer, MA. “Infant crying: An evolutionary perspective.” New Evidence on Unexplained Early Infant Crying: Its Origins, Nature, and Management. Ed. RG Barr, et al. Johnson and Johnson Pediatric Institute: Skillman, New Jersey (2001) 59-70.
Hunziker, Urs, et. al. “Increased Carrying Reduces Infant Crying: A Randomized Controlled Trial.” Pediatrics 77:5 (1986)
Karasik, Lana B. et. al. “WEIRD Walking: Cross-Cultural Research on Motor Development.” Behav Brain Sci. 33:2-3 (2010) 95–96.
Karasik, Lana B. et al. “Places and postures: A cross-cultural comparison of sitting in 5- month-olds.” J Cross Cult Psychol. 46:8 (2015) 1023–1038.
Suskind, Diana, et. al. “The Effect of the Young Child-Carrying Practices of Nigerian Women: on Gross Motor and Language Development in Young Children.” (1998)
