

In the 1950’s sick babies and toddlers at the Cincinnati Children’s Hospital were being fed a chemical called dihydroxyacetone as part of an experiment what developed was sunless tanner.
First, let’s look at the history of the Cincinnati Children’s Hospital and how it came to be involved in research:
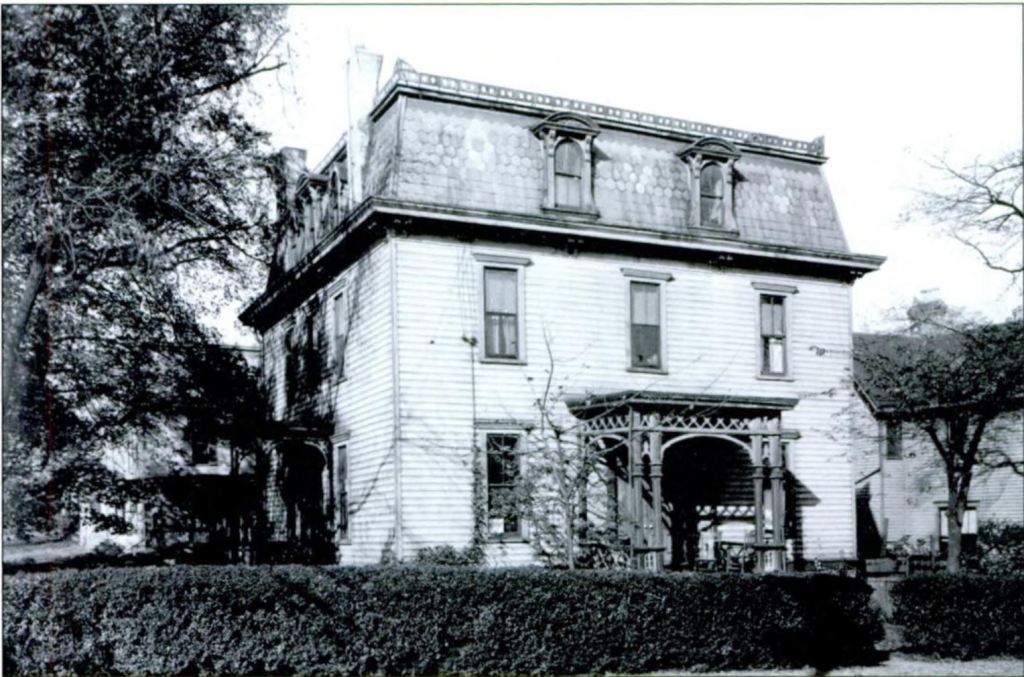
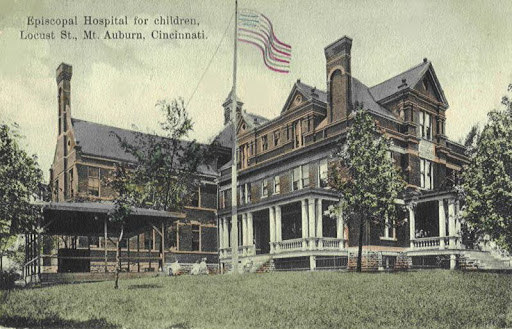
In 1883, Cincinnati Children’s Hospital, originally called the Protestant Episcopal Hospital, began as a philanthropic project Mrs. Robert Dayton, Isabelle Hopkins, and Mary Emory. With the financial support of their Episcopal Bishop, Thomas Jaggar, they opened their hospital, at first a small three-bedroom house (which still stands) in the Walnut Hills neighborhood of Cincinnati, at the corner of Park Ave and Yale Street. They quickly realized the need far outstripped their capacity and in 1887, a new hospital was built on land in Mount Auburn purchased by Thomas and J. Josiah Emery, near Christ Hospital.

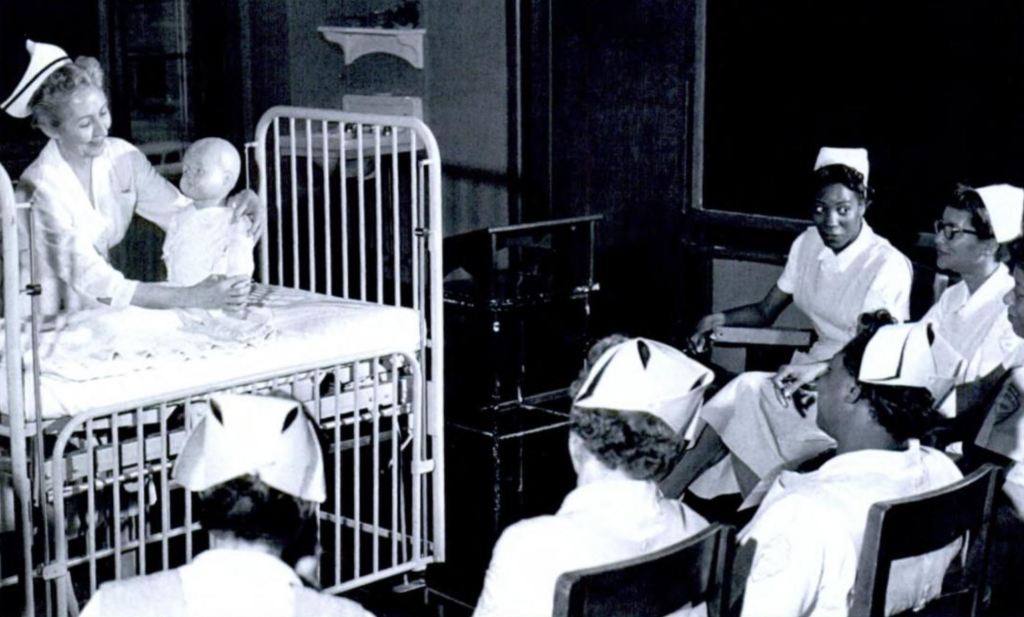
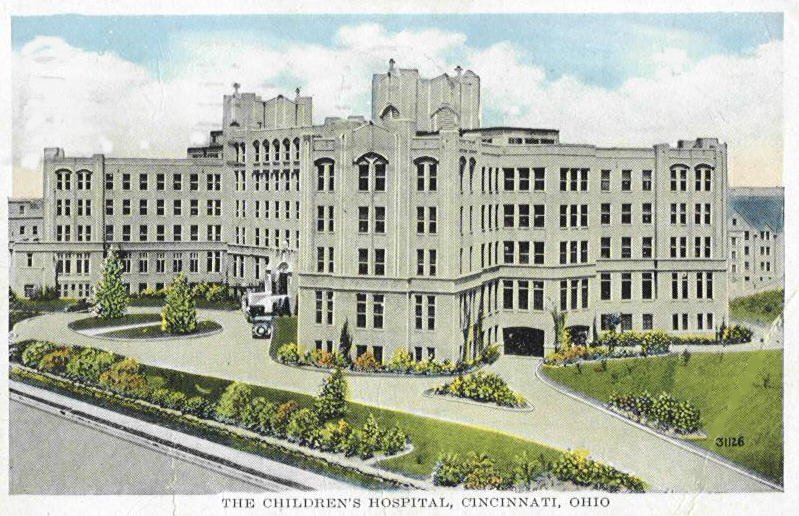
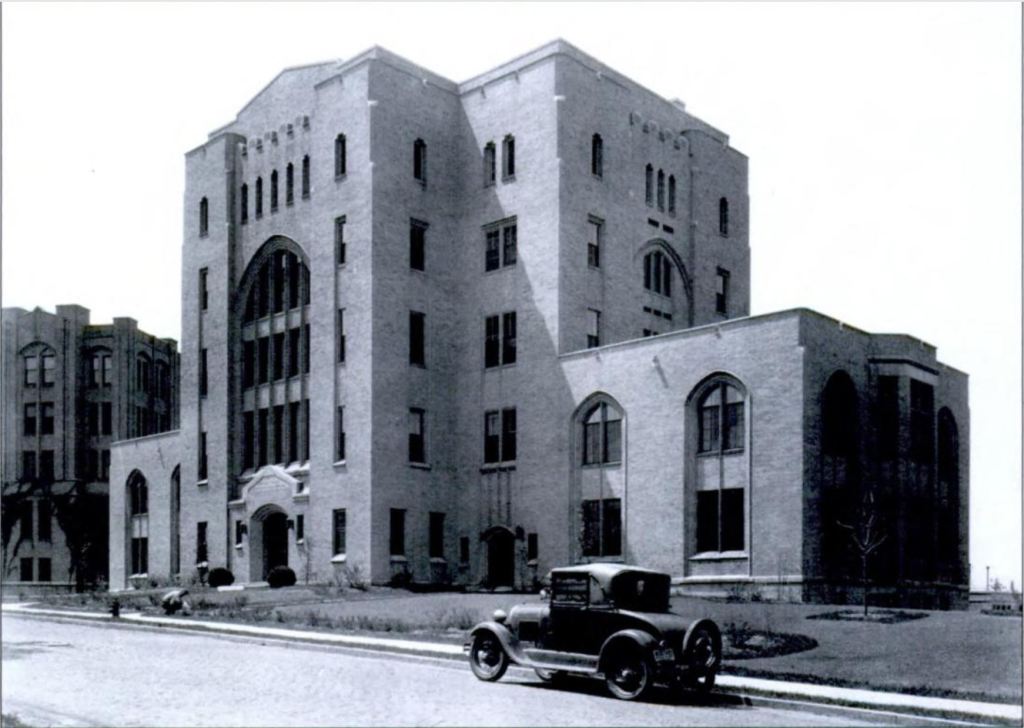
In 1926 the hospital once again moved, this time to a larger 200-bed facility nearer the College of Medicine, becoming established as a department of pediatrics, whose chairman was Dr. A. Graeme Mitchell. It was his goal to start a research facility and after the president of the Hospital Board, William Cooper Proctor donated $2.5 million to build and endow it, The Children’s Hospital Research Foundation was opened in 1931. In 1950, the new chairman of the pediatrics department, Dr. Ashely Weech, added a new research and laboratory wing.
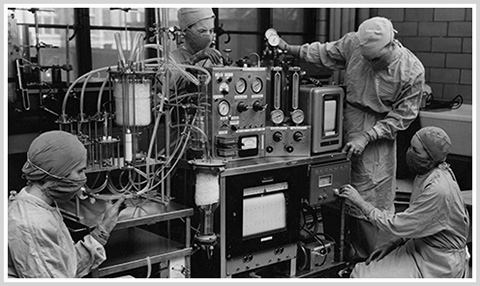
The Cincinnati’s Children’s Hospital produced foundational work in the fields of teratology, the study of birth defects, thanks Dr Josef Warkany, as well as the development of Sabin’s oral polio vaccine; Dr Kaplan, Dr Helmsworth and Dr Clark, developed the first functional heart-lung machine.

Glycogen Storage Diseases
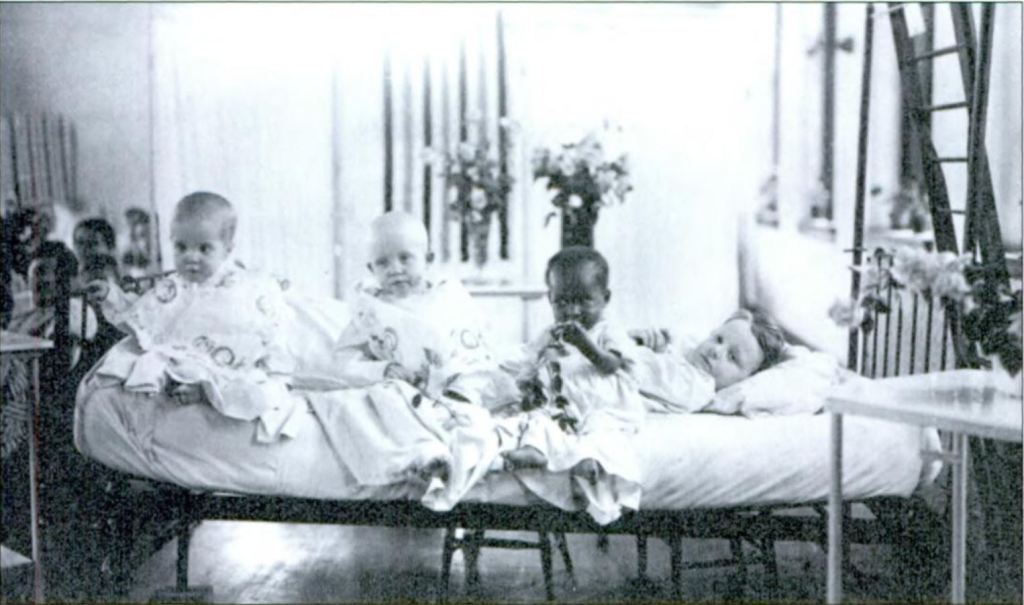
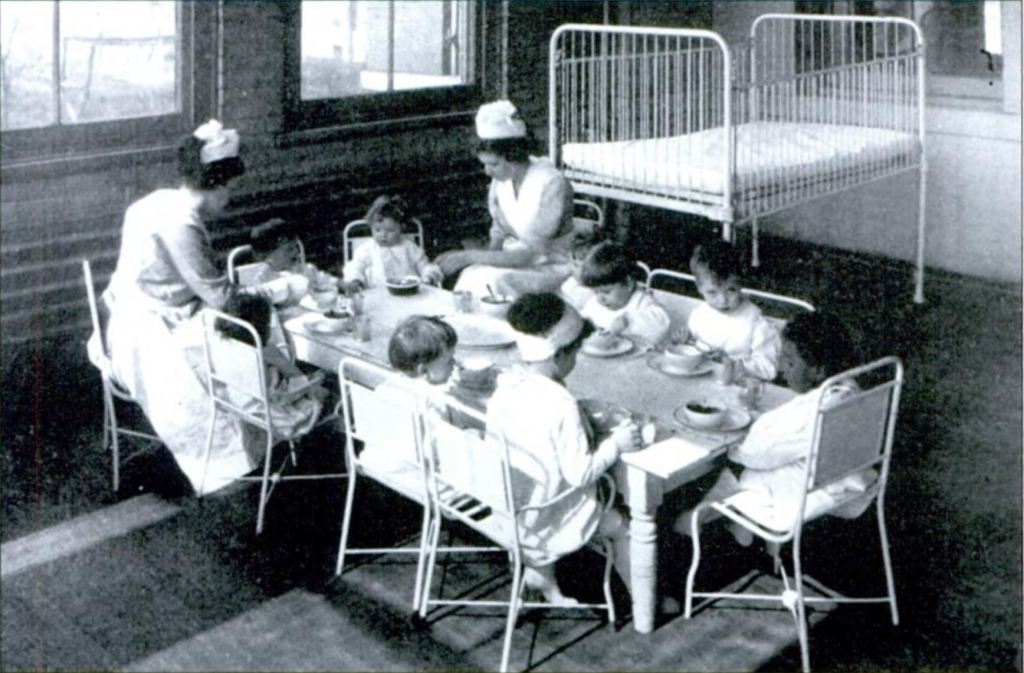
It was in the 1950s at this prestigious children’s hospital and research facility that Eva Wittgenstein was trying to see if a sugar substitute, dihydroxyacetone (DHA), used for diabetics since the 1920s would be safe for babies and children born with glycogen storage diseases.
Glycogen storage diseases (there are a few) are rare and nearly always hereditary (a recessive trait so most parents with the mutation have no idea). It’s congenital meaning they are found in babies and young children (though rarely it can develop in an adult).
These conditions have to do with the way the body uses glycogen, which is the stored form of glucose or blood sugar. Most healthy people have it in our liver and our muscle tissues ready for immediate access during activity. There are many types of GSD but the most common (again, of a rare condition) are types 1, 3 and 4.
- Type I, von Gierke disease, causes the build-up of glycogen in the liver, which is usually caught at 3-4 months of age due to the low blood sugar and swollen belly (caused by the liver) of the baby.
- Type III, Cori disease, or Forbes disease, they lack the debranching enzyme, so glycogen cannot be broken down properly, so it collects in the liver and muscles causing swollen belly, delayed growth and overall weakness.
- Type IV or Andersen disease causes the body to make weird glycogen which triggers an immune response which then causes scarring (or cirrhosis) of the liver and other muscles including the heart. This can eventually lead to liver failure. (John Hopkins.)
There are many symptoms in addition to the ones listed above, including easy bruising, and in infants, blood work may show acidosis (acidic blood) and high cholesterol. Today, special diets and medications, including enzyme replacement therapy are used to help manage this condition but it’s important to catch it as early as possible (there are some links below for more information).
Sugar Substitute
Back to Eva in the 1950s, testing out dihydroxyacetone as a sugar substitute for GSD babies. She had to feed the babies and children relatively large doses of the stuff, 1g per 1kg of body weight, and invariably some of it ended getting splashed or spit back up. That’s when she noticed something strange happening: where the solution landed on their skin, it became stained and orangey-brown yet the clothing had no stains.
I searched high and low for more information on the study with the children. Was this a good sugar substitute for them? No idea. It seems that having witnessed this reaction and even testing it on her own skin, Eva and her colleague Helen Berry, forgot about the kids and got to work studying the effects of the sweetener on skin.

Sunless Tanner
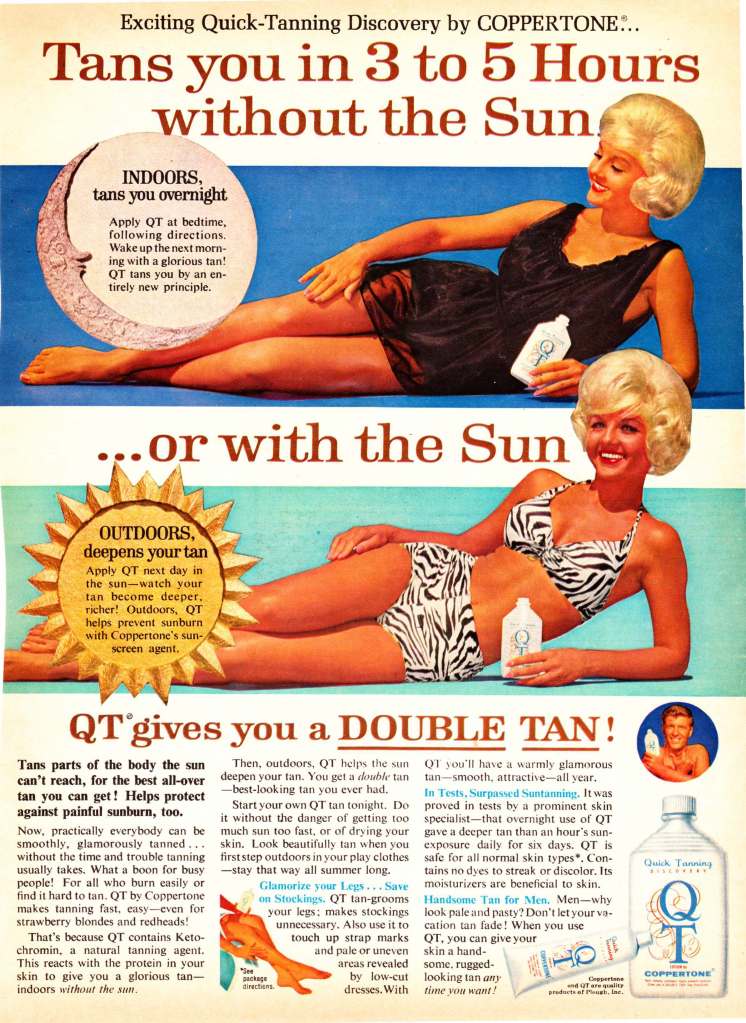
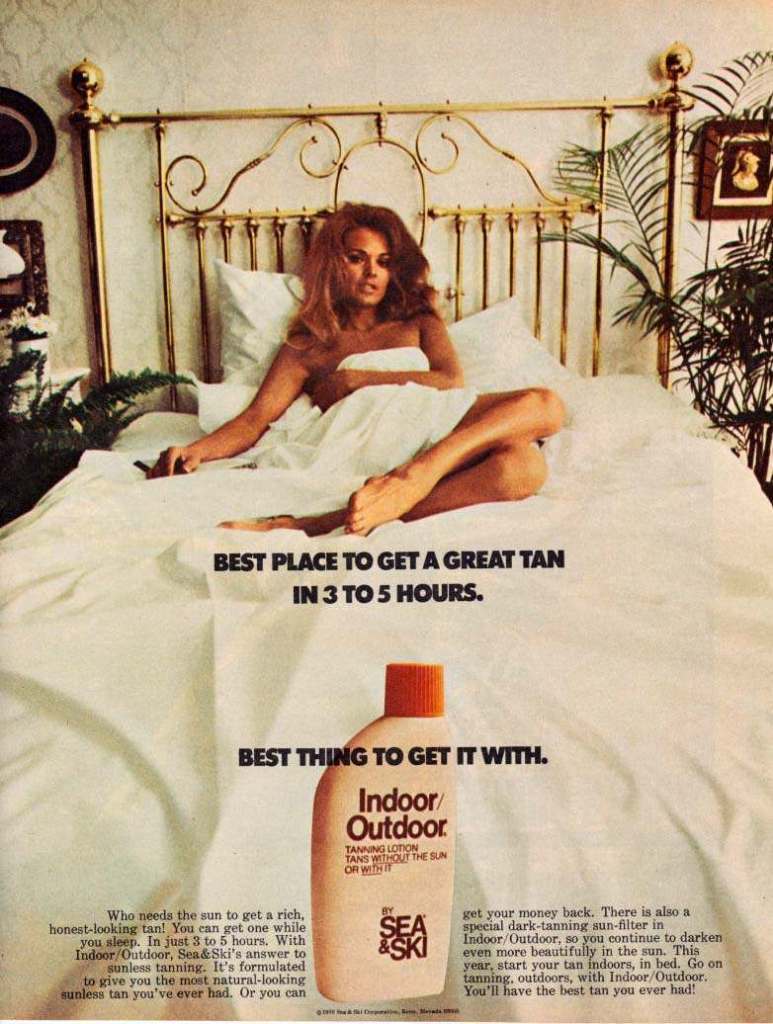
They soon learned that the stain was being caused by a chemical reaction called the Maillard reaction, the same thing that occurs when you brown food or caramelize sugar. It’s caused by the interaction between the dihydroxyacetone and the amino acids in the topmost layer of skin to produce melanoidins. Eva and Helen went on to publish a number of articles examining the reaction in detail which I will link below. By 1970, dihydroxyacetone was being added into lotions sold as sunless tanners. Unlike a lot of products from the 1950s, DHA as a sunless tanner is still considered safe, it’s FDA approved as a colorant for external use.
If you really want to have tan-looking skin and don’t naturally have it, sunless tanners are the only safe option. Tanning beds and laying out in the sun is damaging, it is literally self-harm, and you can die from skin cancer. Even if you use sunless tanners, you still need to use UV protection, a tan from any source does not protect you from further sun damage or skin cancers.
So there you go, how sick babies, with the help of Cincinnati Children’s Hospital, brought the world oompaloom– er– sunless tanners. Don’t forget the sunscreen!
If you would like to support my research, you can share my posts on social media, subscribe on Youtube, Facebook and/or Instagram, or become a patron on Patreon.
Sources:
Cincinnati Children’s Hospital: Glycogen Storage Disorders, webpage.
Cincinnati Children’s Hospital: Our History, webpage.
Katz, Beatrice. 2008. Cincinnati Children’s Hospital Medical Center. Arcadia Publishing.
Library of Congress.
Wittgenstein, Eva and Helen K. Berry. 1960. “Staining of Skin with Dihydroxyacetone.” Science. 30 Sep 1960, 132(3431): 894-895
Wittgenstein, Eva and Helen K. Berry. 1961. “Reaction of dihydroxyacetone (DHA) with human skin callus and amino compounds.” The Journal of Investigative Dermatology, 36:283-6. Full text.
Wittgenstein, Eva and G.M. Guest. 1961. “BIOCHEMICAL EFFECTS OF DIHYDROXYACETONE.” The Journal of Investigative Dermatology, 37: 421-426. Full Text.
Yeoman, Lowbrow. 2015. “Let the Sun Shine In: 1960s-70s Adverts in the Golden Age of the Tan.” Flashbak.
